Simulation of safe and dignified burial for control of Bundibugyo Ebola virus epidemics
This study has not yet been peer reviewed.
The ongoing epidemic of Ebola Bundibugyo Virus Disease (BVD) in the eastern Democratic Republic of Congo (DRC) and Uganda appears to be propagating. Just as during the previous large DRC epidemic (2018-2020), there have been concerning reports of a breakdown in community trust and violence surrounding the burial of hospitalised cases. These reports underscore the importance of ensuring culturally appropriate, accessible, compassionate inhumation of people who die from BVD, the bodies of whom remain infectious after their death.
Safe and dignified burial (SDB) is a recognised pillar of Ebola response and is supported by evidence as a superior alternative to either (i) no support for safe burial, which can result in unchecked propagation; or, perhaps worse still, (ii) militarised, coercive approaches to patient isolation and burial management: these impede grief, worsen mental health, have been shown to result in mistrust and can disincentivise care-seeking [10–13]. At least in DRC, SDB has previously been offered presumptively, i.e. for any deaths in the community regardless of whether they had received an Ebola test or diagnosis.
We use a simple transmission model to explore different scenarios of how SDB could affect the epidemic’s trajectory, and thus inform decisions about which targets the SDB service should set out to achieve. We take as our analysis unit an average-sized health zone in eastern DRC in which SDB is implemented once the outbreak reaches a certain size. We reach the following conclusions:
-
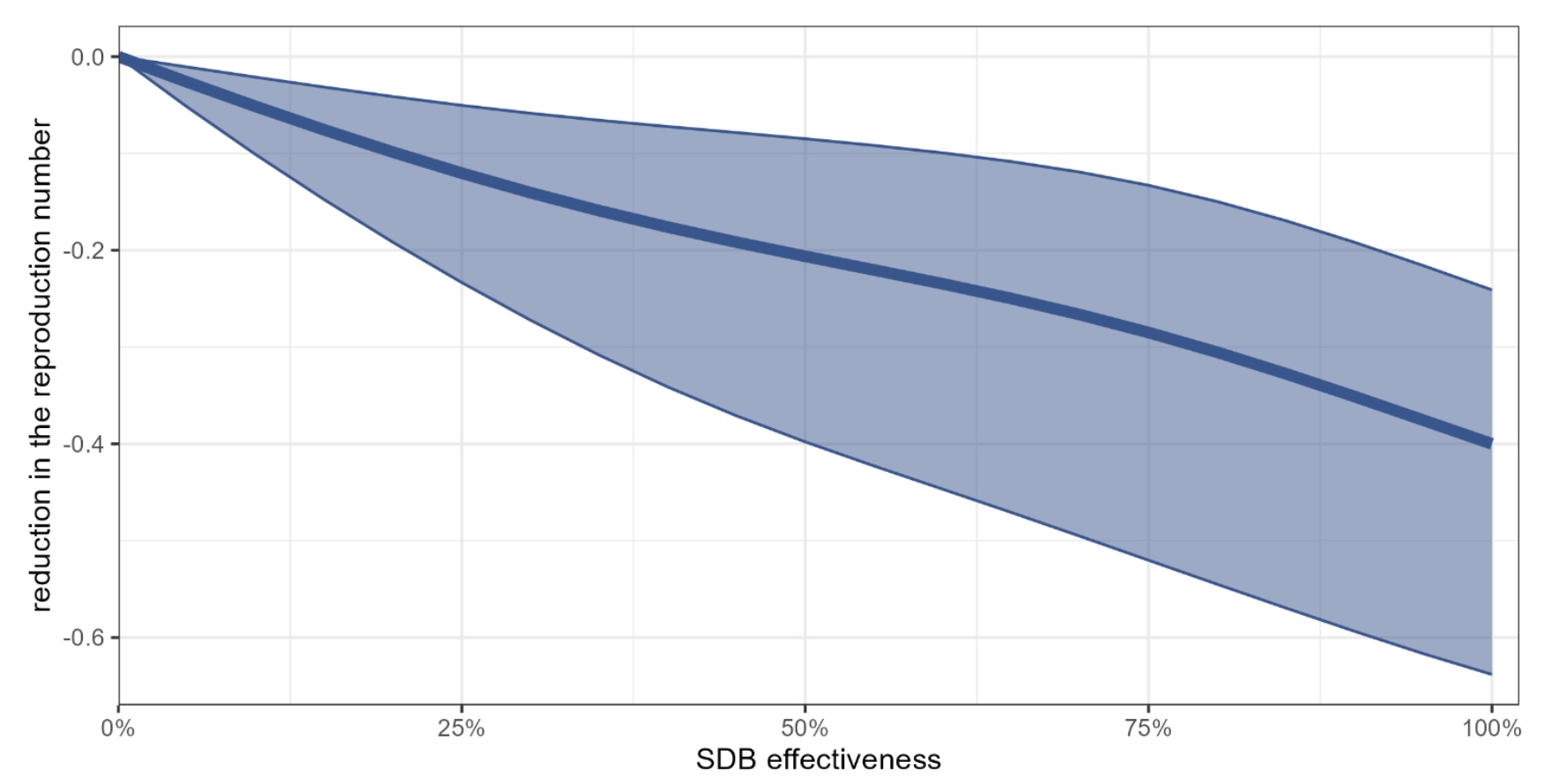
Achieving high SDB coverage and effectiveness is very important, underscoring the need for community engagement and trust-building, as well as strong collaboration between the SDB service and other response pillars (in particular surveillance/contact tracing).
-
Under certain conditions of low transmissibility, SDB could make the difference between outbreak propagation and extinction. The combination of highly performant SDB and, say, isolation and case management would probably make a formidable contribution to transmission. Moreover, SDB as a trust- building measure is likely to encourage care-seeking and case reporting, and could thus act synergistically with other interventions.
-
The longer it takes for SDB to get underway, the harder it will take to bring outbreaks under control. With this in mind, it may be efficient to preposition and activate SDB even in areas where no transmission is yet observed: while we have not explored the spatial dynamics of the epidemic here, such a strategy may prevent geographic spillover.
The full report is available here in English and in French.