Confirmatory testing with a second lateral flow test may mitigate false positives at low levels of SARS-CoV-2 prevalence in English schools
Status: Report | First online: 12 March 2021 | Last update: 12 March 2021
This study has not yet been peer reviewed.
Read the full report here. The R code to reproduce this analysis can be found here.
- There is currently concern over the possibility of false-positive lateral flow test (LFT) results in the mass asymptomatic testing programme in English schools, with calls for positive LFTs to be confirmed by Polymerase Chain Reaction (PCR) tests.
- However, delays in isolating cases and their contacts due to PCR test delays may lead to increased transmission risk and should be avoided unless strictly necessary.
- Here we show that, at current levels of prevalence in schoolchildren (~0.43%), the chance of a positive test being a true positive (Positive Predictive Value, PPV) is high (88%) and prevalence would need to decrease to below 0.05% in order for the number of false-positive test results to outnumber true positives.
- Were prevalence to decrease below 0.05%, a confirmatory LFT would increase PPV to >99.97%, similar to that of a confirmatory PCR (>99.99%).
- Following up an initial positive LFT with a second LFT provides a high PPV, minimises disruption, and enables faster case isolation and contact tracing than a confirmatory PCR test.
- This analysis makes the assumption that LFT test results are independent of each other, which may overestimate the joint specificity and underestimate the joint sensitivity.
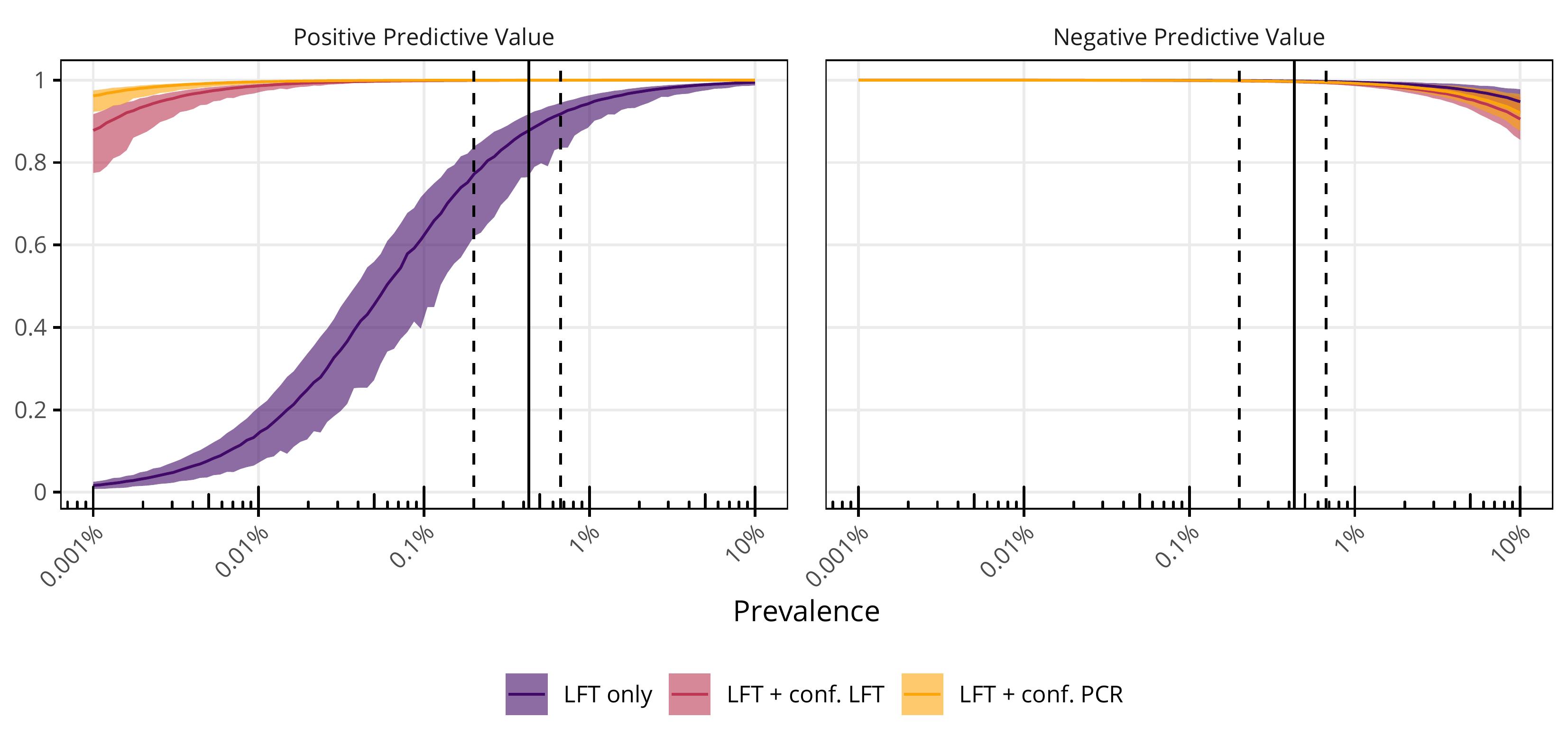
Figure: Positive and Negative Predictive Value for different testing strategies at varying levels of prevalence. Coloured lines and bands indicate the median and 95% CI for PPV and NPV for sampled values of prevalence, assuming the same coefficient of variation as current prevalence estimates. Solid and dashed vertical lines are approximate median and 95% CIs of current SARS-CoV-2 prevalence in school children.